- TMJ
- Biological / Holistic Dentistry
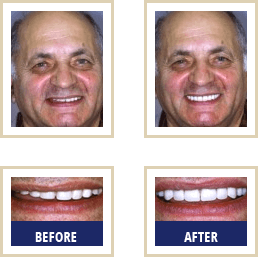
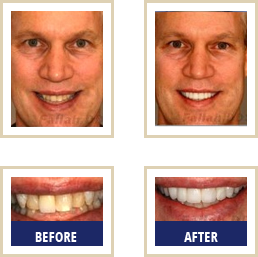
- Smile Makeover / Cosmetic Dentistry
- Zirconium Implants
- Pin Hole Gum Lift
- General Dentistry
Blog
01/13/16
Your Teeth - Your Health
Are your teeth and gums healthy? Their health may be an important indicator of your general health.
More and more research suggests that the same good health and nutritional practices that prevent cavities and gum disease may also keep you healthy and prevent other illnesses.
Research has shown that serious chronic health problems are often associated with dental caries, or cavities, and gum pathology. This connection is documented by a large number of recent studies performed after 1990. For example - poor mental health is associated with cavities [1-4]. In a study published in the Journal of the American Geriatrics Society, January 2008 [1], elderly individuals without dementia were found to have an average of only 2.7 fillings. Elderly individuals with dementia or Alzheimer's disease averaged 7.8 teeth with fillings.
A recent authoritative review showed a clear association between cavities, gum health and heart diseases [5}. Additionally, this same study reported that people with poor oral health, on average, lead shorter lives. Recent publications concerning Periodontal Disease and Your Heart
are listed by the American Association of Periodontology.
You can take this quiz to asses your risk of gum disease:
Gum Health Self-Assessment Quiz.
Connections between diabetes, as well as heart disease, and dental decay have been suspect for decades. Active, ongoing research [6-8] deals with the association between cavities and diabetes. While recent publications concerning Periodontal Disease and Diabetes are listed by the American Association of Periodontology.
A large number of scientists studying this relationship have proposed that diets high in sugar and refined carbohydrates were common cause of these diseases [9-15].
Nutrition is suspect as a possible factor in heart disease, infectious respiratory diseases, dental diseases and mental diseases. These diseases can result, in part, from common failures in metabolism. When a deficiency of essential nutrients occurs, particularly vitamins D, C, and niacin, metabolic failures are inevitable.
The relationship between vitamin D deficiency and cavities is especially strong in dozens of studies conducted in the 1930's and 1940's [16-27]. More than 90% of the studies concluded that Vitamin D supplements prevented children's cavities.
Cancer, respiratory infections, diabetes, heart disease, and other ailments [29] are also linked to a Vitamin D deficiency. For example, a study published in the Archives of Internal Medicine in 2008, indicated that compared to individuals with highest vitamin D levels, individuals with the lowest vitamin D levels had more than double the risk of dying from heart disease and other causes over an eight-year study period. Linus Pauling [15] reviewed evidence for vitamin C was and the evidence for niacin was described by Abram Hoffer [29].
Individuals who ensure their good levels of nutrition through balanced diet and nutrient supplements, in conjunction with good dental care, will have dramatically fewer cavities and gum problems than individuals who only receive good dental care.
References:
[1] B Ellefsen; P Holm-Pedersen; D E Morse; M. Schroll; B. Andersen; G. Waldemar. Caries Prevalence in Older Persons with and without Dementia. Journal of the American Geriatrics Society, Volume 56, Number 1, January 2008, 59-67(9).
[2] J M Chalmers, K D Carter, A J Spencer. Caries incidence and increments in community-living older adults with and without dementia. Australian Research Center for Population Oral Health, Dental School, The University of Adelaide, Adelaide 5005, Australia. Gerodontology Volume 19 Issue 2, 80 – 94.
[3] Friedlander, A.H.; Mahler, M.E. Major depressive disorder psychopathology, medical management and dental implications. Graduate Medical Education, Veterans Affairs Greater Los Angeles Healthcare System (14), Los Angeles, CA, USA. Journal of the American Dental Association (2001), 132(5), 629-638.
[4] Stewart, R.; et. al. Oral Health and Cognitive Function in the Third National Health and Nutrition Examination Survey (NHANES III), Psychosomatic Medicine 70:936-941 (2008).
[5] Meurman, J.H.; Sanz, M.;Janket, S. Oral infection and vascular disease. Institute of Dentistry, University of Helsinki, Finland. Vascular Disease Prevention (2007), 4(4), 260-267.
[6] Touger-Decker R, Sirois D A, Vernillo A T. Diabetes mellitus: Nutrition and oral health relationships. Department of Primary Care, School of Health-Related Professions, University of Medicine and Dentistry of New Jersey, Newark, NJ, USA. Editor(s): Touger-Decker, Riva. Nutrition and Oral Medicine (2005), 185-204.
[7] Diaz-Romero, R.; Casanova-Roman, R.; Beltran-Zuniga, M; Belmont-Padilla, J.; Mendez, J.; Avila-Rosas, H.. Oral Infections and Glycemic Control in Pregnant Type 2 Diabetics. Instituto Nacional de Perinatologia, Mexico City, Mex. Archives of Medical Research (2005), 36(1), 42-48.
[8] Twetman, S.; Johansson, I.; Birkhed, D.; Nederfors, T. Caries incidence in young type 1 diabetes mellitus patients in relation to metabolic control and caries-associated risk factors. Caries Research (2002), 36(1), 31-35.
[9] Bommer, S. Diseases of civilization and nutrition. Ernaehrungsforschung (1963), 7 598-612.
[10] Miler-Sosnkowska, M. Role of dietary carbohydrates in relation to their metabolism. Inst. Zywienia Czlowieka, Akad. Roln., Warsaw, Pol. Postepy Higieny i Medycyny Doswiadczalnej (1975), 29(4), 537-55.
[11] Cremer, H.D.; Eyer, H. Carbohydrates. Inst. Ernaehrungswiss. I, Univ. Giessen, Giessen, Fed. Rep. Ger. Ernaehrungs-Umschau (1975), 22(10), 291-3.
[12] Newberne, P.M.. Nutrition: summary of evidence. Sweeteners: Issues, uncertainties. Acad. Forum, 4th (1975), 76-85, 252-3.
[13] Heraud, G. Sucrose and nutritional pathology. Sucrerie Francaise (1979), 120(24), 21-6.
[14] Nuttall, F.Q.; Gannon, M.C.. Sucrose and disease. Diabetes Care (1981), 4(2), 305-10.
[15] Pauling, L. "How to Live Longer and Feel Better." W.H. Freeman and Company, 1986. Revised 2006, Oregon State University Press.
[16] Tisdall, F.F. The effect of nutrition on the primary teeth. Child Development (1937) 8(1), 102-4.
[17] McBeath, E.C. Nutrition and diet in relation to preventive dentistry. NY J. Dentistry (1938) 8; 17-21.
[17] McBeath, E.C.; Zucker, T.F. Role of vitamin D in the control of dental caries in children. Journal of Nutrition (1938) 15; 547-64.
[19] East, B. R. Nutrition and dental caries. American Journal of Public Health 1938. 28; 72-6.
[20] Mellanby, M. The role of nutrition as a factor in resistance to dental caries. British Dental Journal (1937), 62; 241-52.
[21] His Majesty's Stationery Office, London. The influence of diet on caries in children's teeth. Report of the Committee for the Investigation of Dental Disease (1936).
[22] McBeath, F.C. Vitamin D studies, 1933-1934. American Journal of Public Health (1934), 24 1028-30.
[23] Anderson, P. G.; Williams, C. H. M.; Halderson, H.; Summerfeldt, C.; Agnew, R. Influence of vitamin D in the prevention of dental caries. Journal of the American Dental Association (1934) 21; 1349-66.
[24] Day, C. D.; Sedwick, H. J. Fat-soluble vitamins and dental caries in children. Journal of Nutrition (1934) 8; 309-28.
[25] Agnew, M. C.; Agnew, R. G.; Tisdall, F. F. The production and prevention of dental caries. Journal of the American Dental Association, JADA (1933) 20; 193-212.
[26] Bennett, N. G.; et al. The influence of diet on caries in children's teeth. Special Report Series – Medical Research Council, UK (1931) No. 159, 19.
[27] Mellanby, M.; Pattison, C. L. The influence of a cereal-free diet rich in vitamin D and calcium on dental caries in children. British Medical Journal (1932) I 507-10.
[28] Brodsky, R. H.; Schick, B.; Vollmer, H.. Prevention of dental caries by massive doses of vitamin D. American Journal of Diseases of Children (1941) 62; 1183-7.
[29] Hoffer A, Saul AW. Orthomolecular Medicine for Everyone. Laguna Beach, California, Basic Health Pub, 2008
01/10/16
Choosing a Dentist
When choosing a dentist for you and your family, there are things you should evaluate before you make a decision.
For example, ask yourself the following questions:
Are the dentist and staff personable?
Do they listen to your individual needs and / or goals?
Will they tailor your treatment plan to keep you healthy?
Will they offer you amenities to keep you comfortable and calm?
- oral conscious sedation
- laughing gas
- massage chairs
- ceiling mounted plasma TVs?
- mutual respect in a relationship?
and most importantly
- are they using biocompatible materials to ensure your safety?
Dr. Fallah: "When a patient comes to see us for a consultation we really want to find out what their needs are.
What are you looking for in terms of your dental needs?
What are your expectations?
What are your goals?
Are you looking for routine maintenance?
Do you have pain issues or
are you interested in orthodontia or cosmetic dentistry?
We basically get to know each other and get to be comfortable with each other.
Our goal is to really get in tune with exactly why you are seeking our help.
And then from that, we schedule an appointment for records that are pertinent such as digital x-rays. We'll spend a significant amount of time at the examination appointment to really find out what your options are
and then go from there."
More coming soon on Dr. Fallah's patient-centered, holistic dentistry.
Amalgam Silver Fillings
The holistic approach is a philosophy for ensuring that entire patient is being treated.
Infection
For example: when looking at the patient -- Dr. Fallah deals with infections, whether due to gum disease, mouth problems or an infected tooth.
Dr. Fallah states that he "... checks for infection and makes certain to deal with it in the best possible way - with a biological approach and an approach that is kindest to the patient."
For example: disease can be present without pain to the patient, as with gum disease - when space between gum and tooth opens and bacteria enter.
Without proper cleanings and oral hygiene, the bacterial changes become more anaerobic and the bacteria basically digest and break down the space between the tooth and gum - with no pain to the patient. These bacteria cause a lot of damage without pain and can enter the lymphatic system, the blood system and lodge in the heart, lungs or the brain. More importantly it can create low-grade chronic infections. In addition, there is an infant low birth weight associated with women with gum disease and increases in incidence of heart problems for people with gum disease.
Dr. Fallah states that, "... we want to look at the whole body because there are systemic problems that can affect the mouth as well. If someone has an autoimmune disorder such as Lupus and seeks treatment for jaw pain, the process of the treatment will go slower if the Lupus is not addressed."
Dr. Fallah works with rheumatologists and other health care professionals that deal with systemic aspects of health problems.
Structure
Another important aspect of holistic treatment is the structure of the patient.
If someone has a crooked bite, if the upper jaw is canted, or there are issues with the bite, it can cause problems with the jaw, neck and spine.
If someone has sublaxation in their spine, back problems or structural issues and that individual’s bite is prematurely fixed without dealing with spine issues, that spine imbalance will come back and make the bite unstable.
The holistic approach quite literally considers the entire patient.
Amalgam Silver Fillings
Dental amalgam is made of 50% pure elemental mercury, 35% silver, 13% tin, 2% copper, and a trace of zinc and may be called 'silver fillings', amalgam or alloy. These materials are mixed and once placed in the tooth, the mesh enters a solid state.
The World Health Organization has a set of publications that have reported a significant amount of mercury in human bodies that is coming from the dental amalgam.
The FDA has recently advised against used of amalgam fillings in pregnant women and young children - which is a significant step.
Calgary University looked at effects of very minute levels of mercury to the nerve tissues (the amounts that we would be exposed to with dental fillings) and found that the mercury actually caused the nerve cells to degenerate.
Dr Fallah uses rubber Dam, micro seal and oxygen mask to eliminate any mercury exposure to his patient's during removal of their old silver mercury amalgam.
Porcelains and other composites are new materials that cannot just fix a tooth, but truly restore its function, as well as its natural appearance and youthful beauty. Today's restorations are not only esthetically natural and healthy looking, but they feel and wear surprisingly similarly to natural teeth. Obviously no material is as nice as naturally beautiful and healthy teeth, but teeth repaired by or replaced with new materials come amazingly close.
Call or email (info@dentistryforsandiego.com) Dr. Fallah, your Encinitas Cosmetic Dentist, for more information.
State-of-the-Art Technology
Computerized Digital Accuracy versus Articulation Paper
Dr. Fallah uses state-of-the-art, accurate diagnostic and measurement devices such as the T-Scan II. The T-Scan is a device that virtually eliminates the old "trial and error" approach necessary when articulation paper is utilized in analysis of jaw and tooth pressure and alignment during occlusal measurements.
Dr. Fallah uses this advanced technology to ensure unsurpassed accuracy of occlusal and bite data for his patients -- for the most complex -- and even simplest of dental treatment.
The assessment procedure is extremely efficient. No clumsy or messy articulation paper to deal with. The digital data provides a permanent record and guesswork is eliminated.
The T-Scan's 3-D representations are easy to comprehend and provide easy to interpret data for patients. These concise data and occlusal information can be critical in complex dentistry including measurements required for correct placement of dental implants.
The T-Scan allows corrections to bite issues that have the potential to be associated with loose, shifting teeth or teeth that are overly-impacting each other. Excessive pressures on supporting gum and bone structure can be avoided with biting and chewing loads evenly distributed. This balance helps prevent or overcome issues such as TMJ.
A study was performed in 2007 with results that showed the ineffectiveness and inaccuracies of articulating paper:
Determining a Relationship Between Applied Occlusal Load and Articulating Paper Mark Area - Jason P. Carey*,a,Mark Craigb, Robert B. Kersteinc and John Radked
"Articulating paper mark size has been widely accepted in the dental community to be descriptive of occlusal load. The objective of this study is to determine if any direct relationship exists between articulating paper mark area and applied occlusal load. A uniaxial testing machine repeatedly applied a compressive load, beginning at 25N and incrementally continuing up to 450N, to a pair of epoxy dental casts with articulating paper interposed. The resultant paper markings (n = 600) were photographed, and analyzed the mark area using a photographic image analysis and sketching program.
A two-tailed Student's t-test for unequal variances compared the measured size of the mark area between twelve different teeth (p < 0.05). Graphical interpretation of the data indicated that the mark area increased non-linearly with increasing load. When the data was grouped to compare consistency of the mark area between teeth, a high variability of mark area was observed between different teeth at the same applied load. The Student's t-test found significant differences in the size of the mark area approximately 80% of the time. No direct relationship between paper mark area and applied load could be found, although the trend showed increasing mark area with elevating load. When selecting teeth to adjust, an operator should not assume the size of paper markings, accurately describing the markings' occlusal contact force content."